SUPRIYA GAGIREDDY 42
Hi,I am supriya 8th sem medical student.This is an online elog book to discuss our patients de-identified health data shared after taking his/her/guardians signed informed consent.Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.This E-log book reflects my patient centered online learning portfolia
CHIEF COMPLAINTS
A 48 year old male came with chief complaints of
- Abdominal distention since 2 months
- Bilateral pedal edema since 2 months
-Decreased appetite since 2 months
- Decreased urine output since 1 month
HISTORY OF PRESENTING ILLNESS
Patient was apparently alright 2 months back then he developed abdominal distention which is insidious in onset gradually progressive associated with decreased appetite since then.
Bilateral pedal edema extending upto knee since 2 months , pitting type increased on walking and relieved with rest
Decreased urinary output since 1 month
No h/o fever, cough, breathlessness
Daily routine: He get up at 5 in the morning do his daily activities and go to work at 6 in the morning.He reaches his work place in 15mins which is 5km away from his home. He goes by riding cycle. He has his breakfast 9 in the morning. Do his work and have lunch at 1.Return to home at 8 in the nyt and drinks alcohol 180ml.In the day time he also smokes beedi 1pack per day. He eats rice and curry daily 2times.
PAST HISTORY :
No h/o DM HTN TB asthma epilepsy CVA CAD.
PERSONAL HISTORY :
Mixed diet
Normal apetite
Sleep adequate
Bowel and bladder -regular
Consumes 180ml alcohol occasionally and stopped 1 year back.
Smokes beedi 1 pack per day and stopped 3 months back
GENERAL PHYSICAL EXAMINATION:
Patient is conscious ,coherent and cooperative and well oriented to time, place and person.
moderately built and nourished.
Pallor-absent
Icterus -absent
Cyanosis-absent
Clubbing-absent
Generalised Lymphadenopathy-absent
Edema-bilateral pedal edema present
VITALS:
Temperature - 98.2F
PR :- 95bpm
RR : 22cpm
BP :- 110/70mm Hg
SPO2 :- 98%@RA
GRBS :- 110mg/dl.
SYSTEMIC EXAMINATION
Per abdomen -
Abdominal girth- 93-->91cm
Inspection-
Abdomen is distended , flanks are full, skin is stretched , no visible peristalsis , equal symmetrical movements in all quadrant’s with respiration
Palpation -
No local rise of temperature, no tenderness
All inspectory findings are confirmed by palpation, no rebound tenderness, gaurding and rigidity.
No tenderness , No organomegaly
Fluid thrill present
Abdominal girth- 93-->91cm
Percussion:
Shifting dullness present
Auscultation:
Bowel sounds heard
CVS : S1 and S2 heart sounds heard
CNS: NO focal neurological deficits
RR: BAE Present, normal vesicular breath sounds heard,no adventitious sounds
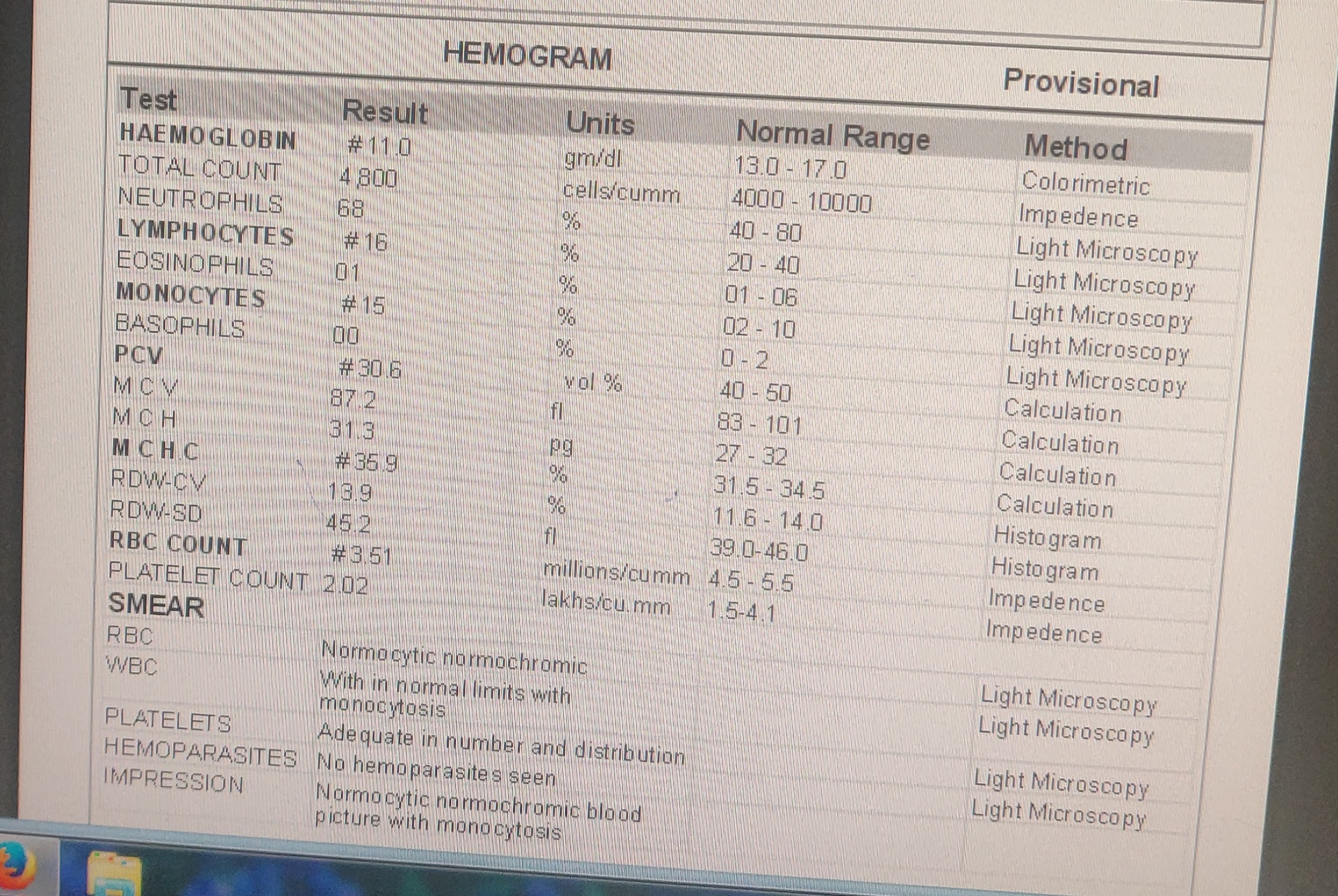
INVESTIGATIONS
Ascitic tap -
Appearance - clear , yellow coloured
SAAG - 1.65 g/dl
Serum albumin - 2.0 g/dl
Asctic albumin - 0.35 g/dl
Ascitic fluid sugar - 104mg/dl
Ascitic fluid protein - 0.7 g/dl
Ascitic fluid amylase - 17 IU /L
LDH : 143 IU/L
Cell count- 50 cells
Lymphocytes nil
Neutrophils 100%.
PROVISIONAL DIAGNOSIS
Chronic liver failure with Ascites?
TREATMENT :
Tab LASIX 40 mg PO BD
Syp. Lactulose 10 ml PO HS
Strict Alcohol abstinence





















Comments
Post a Comment